

Healthcare's Price Is REIT
Profit motives, means and opportunities

Two of capitalism’s hardest circles to square are private prisons and healthcare. It’s not that the profit motive is ill-suited to those enterprises. To the contrary, profit-motivated incarceration and profit-seeking healthcare are excellent ways to generate big returns. The rub is that, like war, the more revenue they generate, the more suffering they seem to cause. In fact, those enterprises—all three of which have developed into industrial complexes—are not only rewarded for ignoring human suffering, but also for causing it. Fifty-eight, largely US-based companies profited from the brutal demolition of Gaza. Money is rolling in to the private prison-keepers at CoreCivic despite the cruel and unusual punishments meted-out at their detention center in Dilley, Texas. There is no financial incentive to invest in frivolities like an actual education for detained kids. Maximum profit comes from providing the bare minimum.
Then there’s the undeniable upside of profit-motivated healthcare, both for investors and the corporate leadership that serves them. For health insurers, it means denial of coverage whenever and wherever they can. Every procedure, office visit, hospital stay and prescription they refuse to cover is money in the bank. For health systems and for-profit hospitals, it’s all about revenue generation. They want high-value procedures and lengthy hospital stays. Pharmaceutical companies want more and more users, and they invent new drugs to treat new conditions. And then there is private equity’s disastrous foray into healthcare. They seek cash cows to milk until they ultimately slaughter them and sell off the steaks.
The profit motive has served them all well.
Perhaps too well.
That’s the message Republicans attempted to embrace when a group of hospital and healthcare system CEOs faced a House Ways and Means Committee searching for “the root causes of rising health care costs in the U.S.” The Hill noted one of the challenges Republicans face now that they’ve decided to flip their script:
The hearings show Republicans are acutely aware that affordability is a top issue among voters ahead of the midterm elections and are willing to show they are holding accountable the corporations and executives they were once allied with.
Ways and Means Chairman Jason Smith (R-MO) set the tone early when he likened the prices the CEOs charge to “borderline extortion." Then the reliably pro-capitalism conservative said this:
“Our local hospitals and physicians have been replaced by mega-corporations that put quarterly earnings over quality care. When hospitals have no competition, it’s no wonder that the sky seems to be the limit for prices.”
The unavoidable fact is that “quarterly earnings” will always trump “quality care,” and Rep. Smith knows it. That’s the nature of the Neoliberal beast unleashed by the Reagan Revolution. The bottom line is the only line that matters. Healthcare is not exempted from Friedman’s Doctrine. And that means a CEO’s sole obligation is to maximize profits for shareholders. Period. End of story.
That cold reality has made healthcare a perennial issue ever since Harris Wofford won a special election for the Pennsylvania Senate seat left vacant by the death of John Heinz in 1991. The Democrat trailed popular Republican Dick Thornburgh by as much as 47 points before pulling off “a shocking 55-to-45 victory.” Guided by the then-unknown duo of James Carville and Paul Begala, Wofford focused on voters’ angst about the cost of healthcare. His solution? National health insurance.
Pollster Mike Donilon explained his candidate’s upset victory to The Washington Post:
From the beginning, voters favored some form of national health insurance by a margin of five to one; 52 percent of them favored it strongly. Donilon tracked this group throughout the campaign and by election day, 65 percent supported Wofford. That suggests that more than 30 percent of the voters picked Wofford on the health care issue alone.
…and…
“People talked about this with a great deal of fear and anxiety,” said Donilon. “These were people who do have health insurance, and fear the choices they could face if they lose it: Do they pay their mortgage, pay their kids’ tuition or pay to take their kid to the hospital?”
That was echoed in a New York Times report on Wofford’s come-from-behind win:
Debbie W. Klotz, a 37-year-old homemaker from York said: “I liked national health care for the simple reason that being unemployed, we are paying our own health insurance, and we can’t afford it, but we can’t afford to do without it.”
And Maryanne O’Brien Donohue, a Scranton homemaker, said, “I really feel this is a time when the Democratic party is representing the middle class.”
Thirty-five years have passed and the Democratic party is once again banking on healthcare to help it reconnect with middle and working class voters. And it probably will, particularly as the impact of Trump’s “One Big Beautiful Bill” is increasingly felt in the months leading up to November. People losing healthcare is a PR disaster and, as evidenced by Rep. Smith hauling CEOs before his committee for a good tongue-lashing, Republicans are desperate to reverse the widespread perception that the GOP aids and abets a health system that still generates “a great deal of fear and anxiety.”
It also generates a lot of anger.
Luigi Mangione became a cult hero when his assassination of United Healthcare CEO Brian Thompson unleashed the pent-up anger many Americans harbor for a system governed by two potentially conflicting mandates: generate profits and deliver healthcare.
Sometimes they align. Oftentimes they do not.
Those conflicting imperatives seem to have genuinely outraged one of Chairman Smith’s Republican colleagues on the Ways and Means committee. A practicing urologist from North Carolina, Representative Greg Murphy is one of twenty physicians currently serving in the 119th Congress. Ironically, though, his epiphany on the problem of profiteering came as a patient.
When Ways and Means held a similar hearing with health insurance executives in January, Rep. Murphy told them of his struggle to get a medication he “needs to exist.”
It took eight denials before insurance agreed.
At the time, he marveled at how difficult the process was for a physician … one who also happens to be a member of Congress. After pondering the plight for Americans who must face similar obstacles without a medical degree or a Congressional staff, he concluded that health insurance was ultimately irredeemable:
[I]f I had it my way I’d turn all of you guys into dust. We’d start back from scratch. We’d have competition in the industry. We’d have association health plans. And we would have nonprofit hospitals rather than profits being put over patients.
Now, with hospital and health system CEOs arrayed before him, the good doctor returned to that theme, but also suggested a new diagnosis, per The Hill:
Rep. Greg Murphy (R-N.C.) asked the chief executive of HCA Healthcare “why we should allow for-profit systems to exist.”
Murphy, a practicing urologist and co-chair of the GOP Doctors’ Caucus, said he understands costs have gone up, and there is uncompensated care.
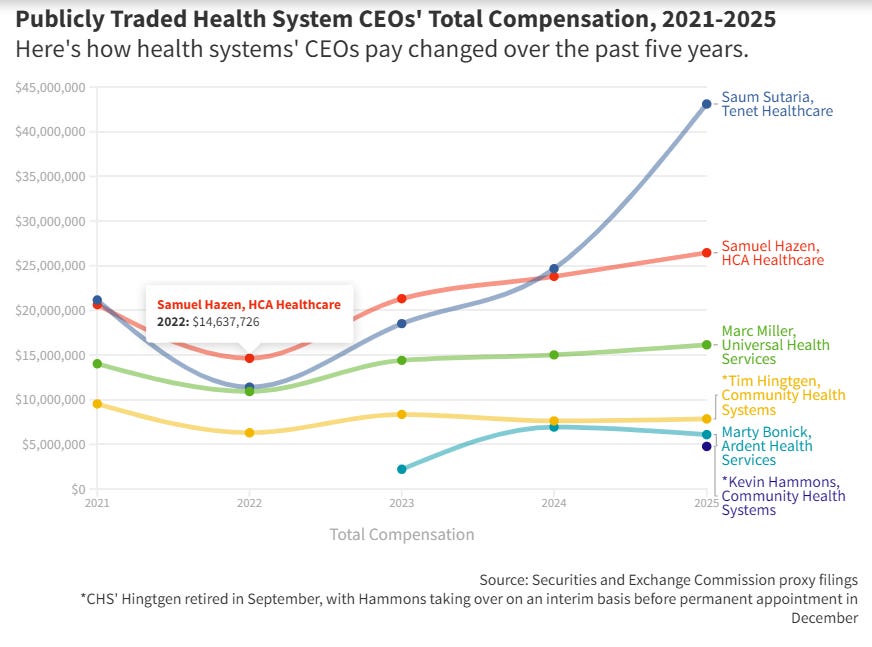
But he noted executive compensation has also risen, and there’s no excuse for companies making exorbitant profits for shareholders who have no connection to health care.
“I don’t want to sound like a communist; I’m not. I’m a capitalist at heart,” Murphy added. “But if we now have institutions that put profits above patients … we have to rethink this model.”
It’s not a matter of “if,” Rep. Murphy.
Institutions regularly put profits above patients.
That’s because the Affordable Care Act effectively enshrined the profit motive in healthcare when it did not eliminate the health insurance industry. It’s probably the main reason it made it through Congress. Imagine the oodles of cash the industry would’ve spent to save itself from elimination under a single-payer system. But it didn’t have to. The ACA was an explicit compromise that preserved capitalistic healthcare.
The law’s architects squared that circle by socializing the inevitable human cost of retaining the profit motive. They did that by expanding Medicaid to cover low-income adults without dependent children and with incomes up to 138% of the poverty line (currently $15,650). For those above the line, it also provided significant, sliding-scale subsidies to those who acquired health insurance through an online ACA exchange. Those compromises became revenue streams for the health insurance industry, but that trade-off also drove the uninsured rate to an all-time low of 7.7% in 2023. That was down from a high of 18.2% in 2010.
Now, thanks to the One Big Beautiful Bill … which Rep. Murphy voted for … that number is likely to swell in 2027 as the first wave of newly ineligible Medicaid recipients is cut loose. They will be joined by up to five million Americans who are beginning to discover insurance is unaffordable without the enhanced subsidies that kept people afloat during the pandemic. In essence, the GOP eliminated the trade-offs that made profiteering tolerable, but also did nothing to address the system’s soon-to-be skyrocketing human cost.
Frankly, Medicaid expansion and ACA subsidies were only Band-Aids. The preservation of the profit motive was destined to produce the perverse incentives currently playing out in Emergency Departments (EDs) around the country as hospital beds are increasingly managed like commercial airline seats. It’s the “terrifying medical underworld” of “emergency room boarding” encountered by the Kaiser Family Foundation’s Elizabeth Rosenthal during her husband’s disastrous end-of-life visits to the ER:
[We] learned the hard way that if you need admission to the hospital, you can remain in the emergency department — in the hallway or a curtained bay on a hard stretcher or in a makeshift holding area — for more than 24 hours, even for days, while waiting for a real hospital bed. In this limbo state, you’re technically admitted to the hospital, but still located in the physical domain of the ER. And the rules governing acceptable care and safety measures become much less clear.
Rosenthal knows of what she speaks…
When I worked as an emergency medicine doctor a few decades ago, the ED was mostly empty at the beginning of my 7 a.m. shift. A few patients might be lingering from the day before: alcoholics who would sober up and leave, patients with a severe burn or a bad case of pneumonia who were waiting for a bed in intensive care.
In the decades since, EDs have doubled or even tripled in size. Even so, patients are piling up. When I started asking around, I quickly discovered ED boarding has become commonplace in the past five or so years and is getting worse, more or less omnipresent in hospitals. “Everyone knows about this problem, and no one cares enough to do anything about it,” Adrian Haimovich, an ED doctor at Boston’s Beth Israel Deaconess Medical Center who studies ED boarding, told me. “It’s barbaric.”
If it’s “barbaric” now, what will it be like when Americans newly priced out of insurance or newly pushed off Medicaid use emergency rooms for health issues preferably handled by an office visit? They will be joined by desperate patients who delayed unaffordable healthcare until an injury or illness becomes life-altering or life-threatening. And they all may end up languishing for hours on a gurney in a hallway:
When I worked as a doctor, if an ED was overwhelmed beyond capacity, the attending (that was me) typically called in to ambulance dispatch to request “diversion” — ambulances should take patients to another hospital. If a hospital got too full, the admitting office canceled elective admissions. Today, hospitals run like airlines and intentionally overbook, Gabe Kelen, the director of emergency medicine at Johns Hopkins University, said. They also have fewer beds than they did a few years ago — in part because nurse (and executive) salaries have risen since the pandemic. An empty, staffed bed is a money loser, so the institution has an incentive to keep beds full and make new patients wait.
What’s more, patients seeking profitable elective procedures are prioritized over those with less remunerative infirmities. Like air travelers, Kelen explained, they get bumped:
“The problem isn’t inefficiency — it’s the way health care finance is structured,” Kelen said. “Hospitals typically run on thin margins. Elective admissions are prioritized because they tend to be for lucrative procedures like heart catheterizations and joint replacements.”
Of course, the house wins whether a patient languishes in the hallway with a less-than lucrative malady or they zip through to pre-op for knee replacement surgery. Here’s Rosenthal’s diagnosis:
Admitting patients through the emergency room has business advantages, too, even if it means they wait for a bed. The evaluation generates charges that typically run many thousands of dollars; once admitted, my husband was still billed the inpatient rate even for a stretcher in the hall. Old, sick, and dying patients are more likely to linger there in part because, after they’re in a real bed, they may take up that spot for days or weeks at a time while waiting for a bed in rehab or hospice, requiring nursing time but not the types of interventions that generate revenue.
If you find yourself old and sick, here’s hoping you require the “types of interventions that generate revenue.” If not, here’s hoping you don’t end up in a REIT-run nursing home like Pearlene Darby:
By the time she was hospitalized in 2020, [the] retired teacher…suffered open sores on both legs, both hips, and both heels, as well as a five-inch-long gash on her tailbone. She died two weeks later at age 81 from infections and bedsores, according to her death certificate. Her daughter sued the nursing home, alleging it had left Darby sitting in her own feces and urine time and again.
The lawsuit, settled on confidential terms last year, blamed not only the managers of City Creek Post-Acute and Assisted Living but also the building’s owner, a real estate investment trust, or REIT.
That’s right. Profit-motivated Real Estate Investment Trusts have quietly moved into the one of the slimier segments of healthcare business—nursing homes.
REITs now own a fifth of the nation’s senior housing, which includes assisted living, memory care, and independent living, according to an industry analysis. REITs also hold investments in 1 in 6 nursing homes. Publicly traded REITs that focus on health care are now worth nearly a quarter of a trillion dollars, according to Nareit, an industry association.
The main allure of investing in nursing facilities is, according to another excellent deep dive by Kaiser Health News, the amazing tax break REITs enjoy :
REITs are required to distribute most of their income and don’t have to pay the 21% federal corporate income tax on it.
That’s quite a break. But there is a “catch.” REITs are forbidden by Federal tax rules from running health care facilities:
A REIT that “directly or indirectly operates or manages” a health care facility loses the tax break for five years.
But this is America. Every new rule or law is just a loophole that hasn’t been opened yet:
Typically, a REIT leases the property to another company that runs the nursing home or assisted living facility and maintains its tax break.
The rub, though, is that REITs are anything but hands-off landlords:
…REITs often select the management who oversee the operations and leave them in place even when they are aware of threadbare staffing, floundering governance, repeated safety violations, or other problems that hamper quality of care.
None of that is a problem, though, if nobody is paying attention:
Despite their ubiquity, REITs remain invisible to state and federal health regulators. Hospitals and nursing homes are not required to disclose rent payments or landlord identities in the annual reports they submit to Medicare.
Even better, the Trump administration scuttled a meager effort to simply let patients know who’s actually running their facility:
Under President Donald Trump, the Centers for Medicare & Medicaid Services indefinitely suspended a Biden-era requirement that nursing homes disclose REIT involvement. Catherine Howden, a CMS spokesperson, said in a statement that the agency does not regulate facilities based on their tax status or corporate form and instead focuses on the quality of the care they provide.
Which brings us back to CareTrust and the REIT model.
Clever capitalists did what clever capitalists are rewarded for doing … they found and exploited a regulatory gap in nursing homes, and they are driving the resulting profits through a gaping a hole in tax law. The only thing they need besides capital (which REITs have in abundance) and regulatory indifference is to find “underperforming” and/or distressed facilities that can be had on-the-cheap.
That was certainly the case with CareTrust.
When they bought the home that would eventually kill Pearlene Darby with a brutal combination of incompetence and indifference, it had a “one-star Medicare rating” and it ”was losing money.”
They got it cheap.
And they got the tax break.
To keep that loophole, CareTrust leased the building to a management company called Kalesta Healthcare Group. But documents show that CareTrust…
…chose the nursing home’s management company and required through the lease that the home keep at least 80% of beds occupied. CareTrust granularly tracked how well the home kept to its financial plan, down to the money spent monthly on nurses and food, the records said. And the documents showed that the real estate company kept tabs on government safety inspection findings and Medicare quality ratings.
When they got those safety inspection findings, though, they didn’t feel the need to improve:
According to a state inspection report, in 2020, the year Darby died, City Creek left a resident in soiled linens “wet from head to toe lying in bed” for more than eight hours. During a different visit, a health inspector cited the home after watching a nurse put a dirty diaper back onto a resident after caring for a wound. “It was just a small stool and it is far from where the wound is,” the nurse told the inspector, according to the report.
Frankly, why would CareTrust spend a dime to improve the conditions at City Creek or any of the facilities in their sprawling empire? They are investors, not doctors or nurses. They are there for the revenue and the tax-free payouts, not to heal the sick or care for the infirm. Their motivation is profit. It may be grim, but they are reaping exactly what they’ve sown:
CareTrust, which now owns more than 500 senior housing and nursing home buildings, reported net income last year of $320 million from $476 million in rents and other revenue — a 67% profit margin. By comparison, HCA Healthcare, one of the nation’s largest for-profit hospital and health care chains, reported a 10% profit margin for last year.
Sixty-seven percent?!?!?
What would it be if the industry prioritized keeping all its residents free of infected bedsores? Fifty-seven percent? Forty-seven percent? Perhaps even thirty-seven percent? Would REITs actually trade a thirty percent reduction in profits for the elimination of preventable deaths from bedsores? Or it is cheaper in the long run to occasionally pay lump sums in lawsuits?
As far as the balance sheet is concerned, there is no difference between the losses incurred from unsuccessfully launching a defective product or failing to regularly turn someone with bedsores. Hell, those payouts are usually tax-deductible, so they practically pay for themselves, anyway. - jp
Here’s what the CEOs and CFOs of public for-profit health systems made in 2025
https://www.fiercehealthcare.com/special-reports/heres-what-ceos-and-cfos-public-profit-health-systems-made-2025
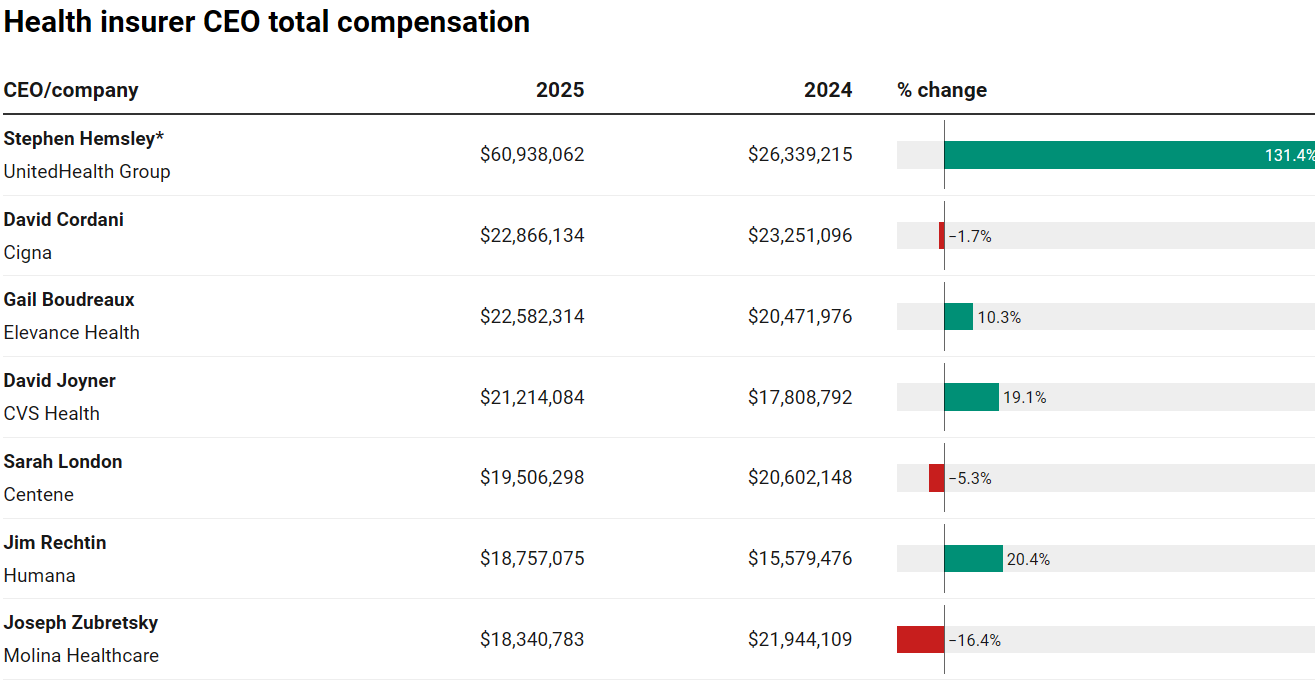
Health insurer CEO pay stagnated as profits faltered in 2025
https://www.modernhealthcare.com/insurance/mh-insurance-ceo-compensation-2025-unitedhealth-humana/
Big Companies Position Themselves for Payday From $50B Federal Rural Health Fund
https://kffhealthnews.org/rural-health/rural-health-transformation-program-cms-state-contractors-ehr-patients/
When care becomes capital: Without urgent safeguards, financialisation risks locking care systems into a race to the bottom
https://www.ips-journal.eu/work-and-digitalisation/when-care-becomes-capital-9021/
REITs Gain Quiet Control Over Nursing Homes as Oversight Lags, KFF Analysis Shows
https://skillednursingnews.com/2026/04/reits-gain-quiet-control-over-nursing-homes-as-oversight-lags-kff-analysis-shows/
Historic nursing home to sell to growing PE firm amid industry pressures
https://www.mcknights.com/news/historic-nursing-home-selling/
Private equity is reshaping Asheville’s vet clinics: ‘They’re circling me like a vulture’
https://avlwatchdog.org/private-equity-is-reshaping-ashevilles-vet-clinics-theyre-circling-me-like-a-vulture/
This is a wonderful article. It should be in the NY Times and in TIME magazine.